 |
|
|
|
Sat, 01 Aug, 2026
|

|

|
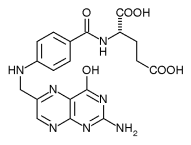
| Folic acid |
 |
| General |
|
Systematic name |
N-[4(2-Amino-4-hydroxy-
pteridin-6-ylmethylamino)-
benzoyl]-L(+)-glutamic acid. |
| Other names |
pteroyl-L-glutamic acid,
Vitamin B9, Vitamin M,
Folacin |
|
Molecular formula |
C19H19N7O6 |
|
SMILES |
C1=CC(=CC=C1C(=O)NC
(CCC(=O)O)C(=O)O)
NCC2=CN=C3C(=N2)
C(=O)N=C(N3)N |
|
Molar mass |
441.40 g/mol |
| Appearance |
yellow-orange
crystalline powder |
|
CAS number |
[59-30-3] |
| Properties |
|
Density and phase |
? g/cm3, solid |
|
Solubility in water |
8.5 g/100 ml (20 °C) |
In ethanol, ether,
acetone |
insoluble |
|
Melting point |
250 °C (523 K), decomp. |
|
Acidity (pKa) |
1st: 2.3, 2nd: 8.3 |
|
Chiral rotation [α]D |
+23°
0.5% in 0.1 M NaOH |
| Hazards |
| Main hazards |
non-toxic, non-flammable |
|
R/S statement |
R: - S: 24/25 |
|
RTECS number |
LP5425000 |
|
UV-Vis |
|
Lambda-max (pH 13) |
259 nm
368 nm |
|
Extinction coefficient (pH 13) |
32340 (259 nm)
7410 (368 nm) |
| Related compounds |
|
Salts |
sodium folate |
Except where noted otherwise, data are given for
materials in their standard state (at 25°C, 100 kPa)
Infobox disclaimer and references |
Folic acid and folate (the anion form) are forms of a water-soluble B vitamin. These occur naturally in food and can also be taken as supplements. Folate gets its name from the Latin word folium, leaf.
 Jump to Page Contents Jump to Page Contents
|
|

Pay as you go
No monthly charges. Access for the price of a phone call
Go>
Unmetered
Flat rate dialup access from only £4.99 a month Go>
Broadband
Surf faster from just £13.99 a month Go> |
Save Even More
Combine your phone and internet, and save on your phone calls
More Info> |
This weeks hot offer
 24: Series 5
24: Series 5
In association with Amazon.co.uk £26.97 |
|
Contents
History
Biological roles
Biochemistry
Recommended Dietary Allowance for folate
Folate deficiency
Folic acid and pregnancy
Folic acid supplements and masking of B12 deficiency
Health risk of too much folic acid
Some current issues and controversies about folate
History - Contents
A key observation of researcher Lucy Wills nearly 70 years ago led to the identification of folate as the nutrient needed to prevent the anemia of pregnancy. Dr. Wills demonstrated that the anemia could be corrected by a yeast extract. Folate was identified as the corrective substance in yeast extract in the late 1930s and was extracted from spinach leaves in 1941.
Biological roles - Contents
Folate is necessary for the production and maintenance of new cells. This is especially important during periods of rapid cell division and growth such as infancy and pregnancy. Folate is needed to replicate DNA and synthesize RNA. It also helps prevent changes to DNA that may lead to cancer. Both adults and children need folate to make normal red blood cells and prevent anemia.
Biochemistry - Contents
In the form of a series of tetrahydrofolate compounds, folate derivatives are coenzymes in a number of single carbon transfer reactions biochemically, and also is involved in the synthesis of dTMP (2'-deoxythymidine-5'-phosphate) from dUMP (2'-deoxyuridine-5'-phosphate).The pathway in the formation of tetrahydrofolate (FH4) is the reduction of folate (F) to dihydrofolate (FH2) by folate reductase, and then the subsequent reduction of dihydrofolate to tetrahydrofolate (FH4) by dihydrofolate reductase.Methylene tetrahydrofolate (CH2FH4) is formed from tetrahydrofolate by the addition of methylene groups from one of three carbon donors: formaldehyde, serine, or glycine. Methyl tetrahydrofolate (CH3–FH4) can be made from methylene tetrahydrofolate by reduction of the methylene group, and formyl tetrahydrofolate (CHO-FH4, folinic acid) is made by oxidation of the methylene tetrahydrofolate.In other words:F → FH2 → FH4 → CH2=FH4 → 1-carbon chemistryA number of drugs interfere with the biosynthesis of folic acid and tetrahydrofolate. Among them are the dihydrofolate reductase inhibitors (such as trimethoprim and pyrimethamine, the sulfonamides (competitive inhibitors of para-aminobenzoic acid in the reactions of dihydropteroate synthetase) and the anticancer drug methotrexate (inhibits both folate reductase and dihydrofolate reductase).
Recommended Dietary Allowance for folate - Contents
The Recommended Dietary Allowance (RDA) is the average daily dietary intake level that is sufficient to meet the nutrient requirements of nearly all (97 to 98 percent) healthy individuals in each life-stage and gender group. The 1998 RDAs for folate are expressed in a term called the Dietary Folate Equivalent (DFE). This was developed to help account for the differences in absorption of naturally-occurring dietary folate and the more bioavailable synthetic folic acid. The 1998 RDAs for folate expressed in micrograms (µg) of DFE for adults are:
Life Stage Men Women Pregnancy Lactation
Ages 19+ 400 µg 400 µg
All ages 600 µg 500 µg
1 µg of food folate = 0.6 µg folic acid from supplements and fortified foods
The National Health and Nutrition Examination Survey (NHANES III 1988-91) and the Continuing Survey of Food Intakes by Individuals (1994-96 CSFII) indicated that most adults did not consume adequate folate. However, the folic acid fortification program in the United States has increased folic acid content of commonly eaten foods such as cereals and grains, and as a result diets of most adults now provide recommended amounts of folate equivalents.
Folate in foods
Leaf vegetables such as spinach and turnip greens, dry beans and peas, fortified cereal products, and some other fruits and vegetables are rich food sources of folate. Some breakfast cereals (ready-to-eat and others) are fortified with 25 percent or 100 percent of the recommended dietary allowance (RDA) for folic acid. A table of selected food sources of folate and folic acid can be found here.
Folate deficiency - Contents
Signs of folic acid deficiency are often subtle. Diarrhea, loss of appetite, and weight loss can occur. Additional signs are weakness, sore tongue, headaches, heart palpitations, irritability, and behavioral disorders. Women with folate deficiency who become pregnant are more likely to give birth to low birth weight and premature infants, and infants with neural tube defects. In adults, anemia is a sign of advanced folate deficiency. In infants and children, folate deficiency can slow growth rate. Some of these symptoms can also result from a variety of medical conditions other than folate deficiency. It is important to have a physician evaluate these symptoms so that appropriate medical care can be given.A deficiency of folate can occur when your need for folate is increased, when dietary intake of folate is inadequate, and when your body excretes (or loses) more folate than usual. Medications that interfere with your body's ability to use folate may also increase the need for this vitamin.,, Some situations that increase the need for folate include:
-
pregnancy and lactation (breastfeeding)
-
alcohol abuse
-
malabsorption, including celiac disease
-
kidney dialysis
-
liver disease
- certain anemias.
Medications can interfere with folate utilization, including:
-
anticonvulsant medications (such as phenytoin, and primidone)
-
metformin (sometimes prescribed to control blood sugar in type 2 diabetes)
-
sulfasalazine (used to control inflammation associated with Crohn's disease and ulcerative colitis)
-
triamterene (a diuretic)
-
methotrexate.
Folic acid and pregnancy - Contents
Folic acid is very important for all women who may become pregnant. Adequate folate intake during the periconceptual period, the time just before and just after a woman becomes pregnant, helps protect against a number of congenital malformations including neural tube defects. Neural tube defects result in malformations of the spine ( spina bifida), skull, and brain ( anencephaly). The risk of neural tube defects is significantly reduced when supplemental folic acid is consumed in addition to a healthy diet prior to and during the first month following conception., Women who could become pregnant are advised to eat foods fortified with folic acid or take supplements in addition to eating folate-rich foods to reduce the risk of some serious birth defects. Taking 400 micrograms of synthetic folic acid daily from fortified foods and/or supplements has been suggested. The Recommended Dietary Allowance (RDA) for folate equivalents for pregnant women is 600 micrograms.
Folic acid supplements and masking of B12 deficiency - Contents
There has been concern about the interaction between vitamin B12 and folic acid. Folic acid supplements can correct the anemia associated with vitamin B12 deficiency. Unfortunately, folic acid will not correct changes in the nervous system that result from vitamin B12 deficiency. Permanent nerve damage could theoretically occur if vitamin B12 deficiency is not treated. Therefore, intake of supplemental folic acid should not exceed 1000 micrograms (µg, sometimes mcg) per day to prevent folic acid from masking symptoms of vitamin B12 deficiency. In fact, evidence that such masking actually occurs is scarce, and there is no evidence that folic acid fortification in Canada or the US has increased the prevalence of vitamin B12 deficiency or its consequences.Still it is important for older adults to be aware of the relationship between folic acid and vitamin B12 because they are at greater risk of having a vitamin B12 deficiency. If you are 50 years of age or older, ask your physician to check your B12 status before you take a supplement that contains folic acid.
Health risk of too much folic acid - Contents
The risk of toxicity from folic acid is low. The Institute of Medicine has established a tolerable upper intake level (UL) for folate of 1,000 µg for adult men and women, and a UL of 800 µg for pregnant and lactating (breast-feeding) women less than 18 years of age. Supplemental folic acid should not exceed the UL to prevent folic acid from masking symptoms of vitamin B12 deficiency.
Some current issues and controversies about folate - Contents
Dietary fortification of folic acid
Since the discovery of the link between insufficient folic acid and neural tube defects (NTDs), governments and health organisations worldwide have made recommendations concerning folic acid supplementation for women intending to become pregnant. For example, the United States Public Health Service (see External links) recommends an extra 0.4 mg/day, which can be taken as a pill. However, many researchers believe that supplementation in this way can never work effectively enough since not all pregnancies are planned and not all women will comply with the recommendation.This has led to the introduction in many countries of fortification, where folic acid is added to flour with the intention of everyone benefiting from the associated raise in blood folate levels. This is not uncontroversial, with issues having been raised concerning individual liberty, and the masking effect of folate fortification on pernicious anaemia (vitamin B12 deficiency). However, most North and South American countries now fortify their flour, along with a number of Middle Eastern countries and Indonesia. Mongolia and a number of ex-Soviet republics are amongst those having widespread voluntary fortification; about five more countries (including Morocco, the first African country) have agreed but not yet implemented fortification. The UK has recently decided not to fortify, mainly because of the vitamin B12 concern; indeed, no EU country has yet fortified.In 1996, the United States Food and Drug Administration (FDA) published regulations requiring the addition of folic acid to enriched breads, cereals, flours, corn meals, pastas, rice, and other grain products., This ruling took effect 1998- 01-01, and was specifically targeted to reduce the risk of neural tube birth defects in newborns. Since the folic acid fortification program took effect, fortified foods have become a major source of folic acid in the American diet. The Centers for Disease Control and Prevention in Atlanta, Georgia used data from 23 birth defect registries that cover about half of United States births and extrapolated their findings to the rest of the country. This data indicates that since the addition of folic acid in grain-based foods as mandated by the Food and Drug Administration, the rate of neural tube defects dropped by 25 percent in the United States.Conversely, in the early 2000s, the US FDA prevented the import of Vegemite from Australia, citing, as the reason, that the folic acid levels are too high. In 2005 it was impossible for Australian Expatriates to buy Vegemite in jars of larger than 113 grams (4 oz.).Although folic acid does reduce the risk of birth defects, it is only one part of the picture and should not be considered a cure. Even women taking daily folic acid supplements have been known to have children with neural tube defects.
Folic acid and heart disease
Low concentrations of folate, vitamin B12, or vitamin B6 may increase your level of homocysteine, an amino acid normally found in your blood. There is evidence that an elevated homocysteine level is an independent risk factor for heart disease and stroke. The evidence suggests that high levels of homocysteine may damage coronary arteries or make it easier for blood clotting cells called platelets to clump together and form a clot. However, there is currently no evidence available to suggest that lowering homocysteine with vitamins will reduce your risk of heart disease. Clinical intervention trials are needed to determine whether supplementation with folic acid, vitamin B12 or vitamin B6 can lower your risk of developing coronary heart disease.
Folic acid and cancer
Some evidence associates low blood levels of folate with a greater risk of cancer. Folate is involved in the synthesis, repair, and functioning of DNA, our genetic map, and a deficiency of folate may result in damage to DNA that may lead to cancer. Several studies have associated diets low in folate with increased risk of breast, pancreatic, and colon cancer. Findings from a study of over 121,000 nurses suggested that long-term folic acid supplementation (for 15 years) was associated with a decreased risk of colon cancer in women 55 to 69 years of age. However, associations between diet and disease do not indicate a direct cause. Researchers are continuing to investigate whether enhanced folate intake from foods or folic acid supplements may reduce the risk of cancer. Until results from such clinical trials are available, folic acid supplements should not be recommended to reduce the risk of cancer.
Folic acid and depression
Some evidence links low levels of folate with depression. There is some limited evidence from randomised controlled trials that using folic acid in addition to antidepressant medication may have benefits. However, the evidence is probably too limited at present for this to be a routine treatment recommendation.
Folic acid and methotrexate for cancer
Folate is important for cells and tissues that rapidly divide. Cancer cells divide rapidly, and drugs that interfere with folate metabolism are used to treat cancer. Methotrexate is a drug often used to treat cancer because it inhibits the production of the active form, tetrahydrofolate. Unfortunately, methotrexate can be toxic, producing side effects such as inflammation in the digestive tract that make it difficult to eat normally.
Folinic acid is a form of folate that can help "rescue" or reverse the toxic effects of methotrexate. Folinic acid is not the same as folic acid. Folic acid supplements have little established role in cancer chemotherapy. There have been cases of severe adverse effects of accidental substitution of folic acid for folinic acid in patients receiving methotrexate cancer chemotherapy. It is important for anyone receiving methotrexate to follow medical advice on the use of folic or folinic acid supplements.
Folic acid and methotrexate for non-cancerous diseases
Low dose methotrexate is used to treat a wide variety of non-cancerous diseases such as rheumatoid arthritis, lupus, psoriasis, asthma, sarcoidoisis, primary biliary cirrhosis, and inflammatory bowel disease. Low doses of methotrexate can deplete folate stores and cause side effects that are similar to folate deficiency. Both high folate diets and supplemental folic acid may help reduce the toxic side effects of low dose methotrexate without decreasing its effectiveness. Anyone taking low dose methotrexate for the health problems listed above should consult with a physician about the need for a folic acid supplement. |
Change Text Size:
[A]
[default]
[A] |




 |
|
|
|
|